
Authors: Joyce Campos, Bhani Sethi, Brianna Gray, Mark Khalil, Leigh Harris, Jasmine Okeagu, Yukta Kulkarni, Hanadi Tajir, Ayania Mayen
Abstract– Medical negligence, argued as both a sociological and ethical concept, is comparable to medical malpractice, with the most defining factor being intent. In the study, the researchers assume medical negligence to be defined as an act where a patient believes he or she could have been treated better after a visit to a doctor or healthcare professional. There are limited studies that focus on racial differences in medical treatment, especially during the Coronavirus (COVID-19/SARS-CoV-2) pandemic. A survey was widely distributed to determine how the treatment of non-white people in a hospital or clinical setting compared to the treatment of white people. The data collected was analyzed and compared to previous studies. In unadjusted results, there were no substantive differences between white and non-white people in the treatment they’ve received since the COVID-19 pandemic expanded. An interesting takeaway from the survey results was the increase in responses indicating that minorities felt satisfied with any medical or clinical treatment received after the pandemic reached the United States. This implies that after the pandemic, there is a decrease in medical insecurity within minority groups.
Keywords-medical negligence, medical insecurity, Coronavirus, minorities, racial differences
Introduction
According to David Guogen J.D., medical negligence is an act or omission by a medical professional that deviates from the accepted medical standard of care (Goguen, 2019). The popular belief is that non-white people endure medical negligence more often than white. Per recent studies announced during the virtual House Committee hearing by the committee of Energy and Commerce on Wednesday, June 17, 2020, regarding the racial and ethnic disparities in the healthcare system during the pandemic, minorities are overrepresented in COVID-19 mortality data. Across 40 states, white Americans are dying from COVID-19 at a rate of 22.7 deaths per 100,000 in the population, whereas African Americans die at a rate of 54.6 deaths per 100,000, Hispanic Americans at a rate of 24.9 deaths per 100,000, and Asian Americans at 24.3 deaths per 100,000 (U.S. Census Bureau, 2010). Apart from disproportional COVID-19 morbidity and mortality rates, hospitals are found to demonstrate differences in care when treating minorities. Dr. Jha, professor of Health Policy and Management at Harvard T. H. Chan School of Public Health, has found that, overall, patients are less likely to recommend minority-serving hospitals than other hospitals and give minority-serving hospitals a high rating (Figueroa et al., 2016). He also found that minority-serving hospitals perform worse than other hospitals on patient care in general, regardless of race.
Events of medical negligence can escalate to court cases, becoming medical malpractice cases. Politically, some barriers prevent certain groups of people from seeking compensation after being racially profiled or discriminated against in a medical or clinical setting. One such barrier is the North Carolina Tort Reform of 2011, a North Carolina bill that makes it more difficult for plaintiffs from lower-income communities to be guaranteed justice. These reforms have resulted in the systematic devaluation of lower-income plaintiffs as lawyers are forced to consider the probability of recovering significant economic damages as the measure for a successful claim (Goodheart, 2018)]. Strong correlations exist between race and socioeconomic status where minorities are more likely to exist in lower socioeconomic levels compared to white people (LaVeist, 2005; Iceland, 2006). The 2010 U.S. Census reports that minorities make roughly half of the population in the three most impoverished towns, determined by per capita income and median household income, in North Carolina: Robeson, Hyde, and Tyrrell (U.S. Census Bureau, 2010). Each town has a substantial population of minorities: Robeson County with 70.55%, Hyde County with 39.60%, and Tyrrell with 43.53% (U.S. Census Bureau, 2010).
Available demographic information from the U.S Census Bureau and political barriers that prevent minorities from seeking compensation from maltreatment, racial profiling, and discrimination in a medical or clinical setting induce the belief that minorities (non-white) suffer from medical negligence much more than white people. The morbidity and mortality rates of minorities during the pandemic also fuel the belief that there is a hidden disparity in the medical realm that separates minorities from white people. The researchers hypothesize that the standard of care toward minorities has worsened, and medical negligence toward minorities has risen since COVID-19 erupted in the United States. There is plenty of research that delves into this racial disparity in the medical world, but there are only a few studies that research this disparity in the setting of the new world with the COVID-19 pandemic.
Materials and Methods
-Study Population
The population in this study consists of people from the tri-state area (New York, New Jersey, and Connecticut). The population was random (n= 122) with an age range spanning from under the age of 8 years and over the age of 55. All children under the age of 18 participated in the study under parental supervision. A trinary system was placed where participants could identify as “Male,” “Female,” or “Other.”People of all races participated: White, Black, American Indian or Alaska Native, Asian, Native Hawaiian or Pacific Islander, Multiracial, and Other. For the purpose of this study, all races other than “white” are considered minorities. Participants varied in employment, educational, and economic statuses.
-Survey Instrument
A Google survey was created and divided into two sections. The first section focused on obtaining demographic data from the participants. Questions regarding gender, age, race, ethnicity, as well as academic, employment, and financial background were included. The second section pertained to any changes COVID-19 had on the participants medically. Questions regarding healthcare coverage, racial profiling, and whether or not they have experienced an instance where the participants believed they could have been treated better were included. These questions were asked twice, both in a before and after instance, and time span since the participant had last seen a doctor or healthcare professional was included. All questions were in the form of multiple choice. A confidentiality disclaimer was included at the top of the survey that explained the survey was to be completed in anonymity, along with the intentions of the lab and who the researchers were. The survey was advertised by means of social media platforms (Facebook and Instagram) and acquaintances, and data was collected for 19 days (t=19).
-Statistical Analysis
Responses to all the questions were collected and compiled into Microsoft Excel. The data that identified the participants (section one) was displayed in single bar graphs individually per identification factor (race, economic status, etc.). The data that was collected regarding the second section of the survey was displayed into double bar graphs that compared the answers of minorities and white participants. Multiple Chi-square tests were conducted on the collected data to determine if there was a significant difference in hospital negligence experienced between minority and white participants. Individual comparisons were made between participants that felt racially profiled before and since COVID-19; similarly for the data that was collected on whether or not the participants felt they would have received better medical care if they belonged to a different race or ethnic group. Comparisons between the answers before and since the COVID-19 outbreak were made as well.
Results
The majority of responses recorded were from participants who live in the New York state area. An overwhelming majority of participants identify either as students or people who are currently employed, with a majority of the participants being 18-24 years old. Backgrounds in education and household incomes, as well as age, varied greatly, compared to gender identification, of which almost a quarter identified as males and the rest identified as females, as shown in figure 1.
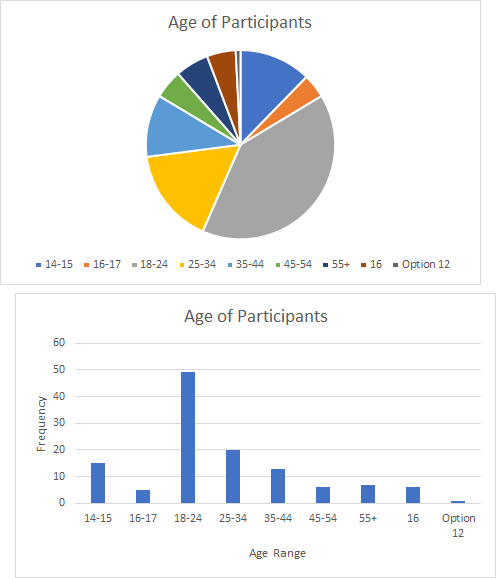


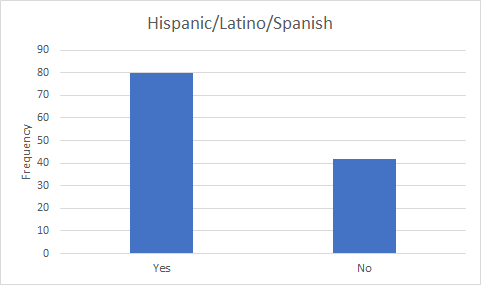
Figure 1.1
These four charts describe the age, gender, and ethnicity of the participants. The majority of participants were 18-24 years old and were female. There was an approximately equal spread of Asian, Black, White, and Other ethnicities, with a lower amount of American Indian/American Native and Multiracial ethnicities. Furthermore, around 80 people identified as Hispanic/Latino/Spanish, and around 40 people did not.
Responses on whether or not the participant felt racially profiled before COVID-19 were gathered. As shown in figure 2, 16.4% of the responses were from Black (non-Hispanic) participants: 5% answered “not sure,” 45% answered “yes,” and 50% answered “no.” 20.5% of responses were from the white (non-Hispanic) participants: 4% answered “not sure,” 12% answered “yes,” and 84% answered “no.” 34.4% of the responses were from Hispanic participants: 31% answered “not sure,” 16.7% answered “yes,” and 52.4% answered “no.” 17.2% of the responses were from Asian (non-Hispanic) participants: 28.6% answered “not sure,” 14.3% answered “yes,” and 57.1% answered “no.” Multiracial participants contributed 3.3% of the responses, with 25% answering “not sure,” another 25% answering “yes,” and 50% answering “no.” Participants that chose “other” contributed 8.2% of the responses, with 20% answering “not sure,” 30% answering “yes,” and 50 % answering “no.” No responses from Native American participants were recorded.


Figure 1.2
The graph on the left represents the number of people overall who believed they experienced racial profiling in a healthcare setting before the COVID-19 outbreak. The graph on the right represents the number of people who believed they experienced racial profiling in a healthcare setting, organized into minorities and white people. The majority of the people in all three groups (yes, no, and note sure) were minorities.
Responses on whether or not the participants felt racially profiled since COVID-19 were gathered. As shown in figure 3, 16.4% of the responses were from Black (non-Hispanic) participants: 40% answered “not sure,” 5% answered “yes,” and 55% answered “no.” 20.5% of responses were from the white (non-Hispanic) participants: 4% answered “not sure,”4% answered “yes,” and 92% answered “no.” 34.4% of the responses were from Hispanic participants: 35.7% answered “not sure,”4.8% answered “yes,” and 59.5% answered “no.” 17.2% of the responses were from Asian (non-Hispanic) participants: 38.1% answered “not sure,” none answered “yes,” and 61.9% answered “no.” Multiracial participants contributed 3.3% of the responses, with none answering “not sure,” none answering “yes,” and 100% answering “no.” Participants that chose “other” contributed 8.2% of the responses, with none answering “not sure,” 30% answering “yes,” and 70% answering “no.” No responses from Native American participants were recorded.


Figure 1.3
The graph on the left represents the number of people, overall, who believed they experienced racial profiling in a healthcare setting since the COVID-19 outbreak. The graph on the right represents the number of people who believed they experienced racial profiling in a healthcare setting, organized into minorities and white people. The majority of the people in all three groups (yes, no, and note sure) were minorities.
Responses on whether or not the participant believed he or she would have received better treatment during their last visit to a doctor or healthcare professional if they were of a different race before COVID-19 were recorded. As shown in figure 4, 23% of the responses were from Black (non-Hispanic) participants: 60.7% answered “not sure,” 28.6% answered “yes,” and 10.7% answered “no.” 23% of responses were from the white (non-Hispanic) participants: 17.9% answered “not sure,” 10.7% answered “yes,” and 71.4% answered “no.”18.9% of the responses were from Asian (non-Hispanic) participants: 43.5% answered “not sure,” 8.7% answered “yes,” and 47.8% answered “no.” Native Americans contributed to 2.5% of the responses: 66.7% answered “not sure,” none answered “yes,” and 33.3% answered “no.” Multiracial participants contributed 9% of the responses, with 18.2% answering “not sure,” another 36.4% answering “yes,” and 45.5% answering “no.” Participants that chose “other” contributed 23.8% of the responses, with 10.3% answering “not sure,” 24.1% answering “yes,” and 65.5% answering “no.” No responses from Hispanic participants were recorded.
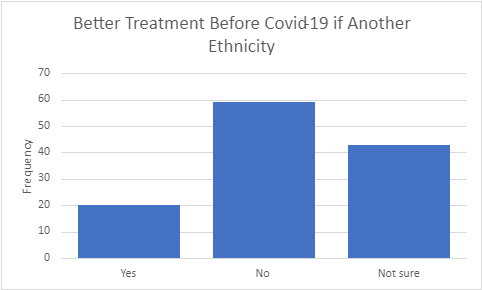

Figure 1.4
The graph on the left represents the number of people overall who believed they would experience better treatment if they were a different ethnicity before the COVID-19 pandemic. The graph on the right represents the number of people who believed they would experience better treatment if they were a different ethnicity before the COVID-10 pandemic, organized into minorities and white people. The majority of the people in all three groups (yes, no, and not sure) were minorities.
Responses on whether or not the participant believed he or she would have received better treatment during their last visit to a doctor or healthcare professional if they were of a different race since COVID-19 were recorded. As shown in figure 5, 23% of the responses were from Black (non-Hispanic) participants: 46.4% answered “not sure,” 3.6% answered “yes,” and 50% answered “no.” 23% of responses were from the white (non-Hispanic) participants: 7.1% answered “not sure,” 3.6% answered “yes,” and 89.3% answered “no.” 18.9% of the responses were from Asian (non-Hispanic) participants: 34.8% answered “not sure,” none answered “yes,” and 65.2% answered “no.” Native Americans contributed to 2.5% of the responses: none answered “not sure,” none answered “yes,” and 100% answered “no.” Multiracial participants contributed 9% of the responses, with 18.2% answering “not sure,” none answering “yes,” and 81.8% answering “no.” Participants that chose “other” contributed 23.8% of the responses, with 24.1% answering “not sure,” 17.2% answering “yes,” and 58.6% answering “no.” No responses from Hispanic participants were recorded.


Figure 1.5
The graph on the left represents the number of people overall who believed they would experience better treatment if they were a different ethnicity since the COVID-19 pandemic. The graph on the right represents the number of people who believed they would experience better treatment if they were a different ethnicity since the COVID-10 pandemic, organized into minorities and white people. The majority of the people in all three groups (yes, no, and not sure) were minorities.
A Chi-square test was conducted on the collected data to determine if there was a significant difference in hospital negligence experienced between minority and white participants. Data from participants who responded that they were unsure whether or not they had experienced hospital negligence before or since COVID-19’s onset were left out from the Chi-square analysis. This was also true for the data set for those who believed that there was an instance where the participant could have gotten better medical care if they were of a different race or ethnic group before or after COVID-19’s onset. The p-value for those who believed that they were racially profiled in a healthcare setting before COVID-19 is 0.270275. The p-value for those who believed that they were racially profiled in a healthcare setting after COVID-19’s onset is 0.440501. The p-value for those who believed that they would have gotten better medical care if they were of a different race or ethnic group is 0.174861. The p-value for those who believed that they would have gotten better medical care if they were of a different race or ethnic group is 0.7763122. These values were all more than the alpha value of 0.05. However, this changes as we analyze the responses of minorities who felt racially profiled in a healthcare setting before and after COVID-19’s onset. The p-value from the Chi-square test for this comparison is 0.029148, less than the alpha value. Finally, the p-value for the minorities who believed that they would receive better quality of care in medical treatment if they were of a different race before COVID-19 compared to after its onset is 0.112584, larger than the alpha value.
Discussion
–Interpretation of the Results and Implications
A public health research study was conducted, determining if and how the standard care for minorities was affected by the COVID-19 pandemic. This was done by surveying participants and collecting data on their beliefs on how they were treated in a healthcare setting. This data was organized and analyzed in four separate ideas: if minorities and white people were racially profiled before and since the COVID-19 pandemic, and if minorities and white people believed they would experience better treatment in a healthcare scenario if they were of a different ethnicity before and since the COVID-19 pandemic. Four chi-square tests were conducted to determine if there was a significant difference between minorities and white people for each of the four questions. The null hypothesis for these questions is that there is no difference between white patients and minorities when it comes to hospital negligence experienced before and since the COVID-19 pandemic, while the alternative hypothesis is that there is a difference between white people and minorities relating to the hospital experience. 2 other chi-square tests were conducted to determine if there was a difference in treatment of minorities and if they felt that they could have been treated better if they had been of a different racial background before and since the COVID-19 pandemic. The null hypothesis for these questions is that there is no difference between before and since the COVID-19 pandemic with regards to hospital negligence experienced. The alternate hypothesis is that there is a difference between the two periods.
The responses for the section regarding racial profiling before COVID-19 in a healthcare environment revealed that both white people and minorities felt that they were not being racially profiled. The majority of the minorities believed that they were either not racially profiled or they were unsure if they were. The majority of white people indicated they have not experienced racial profiling. A chi-square statistic test was conducted to determine if there was a difference in the number of white people or minorities who felt racially profiled before the pandemic. The test resulted in a p-value of 0.270275, which is less than the alpha value of 0.05, indicating that there is no significant difference between the perceived treatment of white people and minorities in a healthcare setting. The null hypothesis, minorities, and white people experience racial profiling in an equal amount in healthcare environments before COVID-19 cannot be rejected. The same analysis was done after COVID-19’s onset, resulting in a p-value of 0.440501, less than the alpha value. The null hypothesis, in this case, minorities and white people experience racial profiling in an equal amount in healthcare environments after COVID-19’s onset, also cannot be rejected. This could suggest that the healthcare system was unbiased in treatment plans and provider-patient interactions before and after the pandemic. However, since the sample size was relatively small, this data is not too reliable.
The responses for the pre-pandemic section on the belief of receiving better treatment if they were of another race revealed that minorities leaned more toward the “no” and “not sure” responses, indicating that plenty of minorities that participated either felt satisfied with any medical or clinical attention received or that more could have been done to satisfy them; whereas the majority of white participants strongly indicated that they were satisfied with any medical or clinical attention received. Comparing the responses to the section regarding the same question, but after the pandemic expanded, there is a rise in the number of minority participants that answered “no,” assuring that they felt like they received nondiscriminatory treatment. This indicates that a majority of minorities strongly felt satisfied with any medical or clinical attention received. Any responses submitted by white participants changed minimally. A chi-squared test was also conducted with this data to determine if there were any significant differences in whether minorities and white people felt that they were receiving nondiscriminatory healthcare treatment. The p-value for the chi-square test pitting minorities against white people with regards to whether or not they felt that they would have received better treatment if they were a different race before COVID-19 was 0.174861, less than the alpha value. The same comparison was done to see if anything changed after COVID-19’s onset. The p-value for this was 0.776312, also less than the alpha value. This confirmed that there were no proven differences between minority groups and white people regarding if they felt that they would have received better treatment if they had been of a different ethnic group before or after COVID-19’s onset.
The results imply that, although minorities tend to suffer higher morbidity and mortality rates during the COVID-19 pandemic, there is no significant degree of medical negligence occurring toward minorities compared to the white patients before or after COVID-19’s onset. However, minorities felt that they were experiencing a difference in treatment before compared to after COVID-19’s onset. Instead of the data proving the researchers’ hypothesis that there was a negative change in the treatment of minorities after COVID-19’s onset compared to before, there was actually a positive change found. Minorities experienced less hospital negligence after COVID-19’s onset. This is all proven through the chi-square test conducted on the survey responses of minorities on whether they had experienced racial discrimination in a healthcare setting before vs. after COVID-19’s onset. The p-value generated, 0.029148, less than the alpha value. The null hypothesis that minorities were treated the same before and after COVID-19’s onset is rejected.
–Limitations of Study
The limitations of the research consist of having insufficient responses and data for the second section of the survey questioning participants’ medical experiences during the pandemic. The results were collected during Summer 2020; the collection of survey responses towards the latter end of the pandemic before vaccinations were introduced could have been beneficial. This would have possibly given minorities more time in healthcare environments, contributing to a difference in responses. A broader range of participants in other areas apart from the Northeast would contribute more to the study, reducing bias. Another limitation is the possibility that participants were less inclined to seek medical treatment during the pandemic. Research from Wong LE et al. reveals that patients with medical emergencies are avoiding the emergency department because of fear of contracting COVID-19 (Wong et al., 2020). This takes away from the researchers’ target audience. More studies can confirm or contradict the researchers’ findings.
Conclusion
The Chi-square tests showed that there is no significant difference between medical negligence and minorities before or after the onset of COVID-19, contradicting the researchers’ hypothesis. As a matter of fact, minority groups felt that they were being treated better in healthcare environments after the beginning of the pandemic as compared to before, according to the survey. Future research with a larger and more diverse sample size may build onto the findings. Prior studies reveal that COVID-19 morbidity and mortality vary across the country but have one trend in common: older male Black people are hospitalized at the highest rate (Gold et al., 2020; Garg et al., 2020; Qing-Xia et al., 2020; Petrilli et al., 2020). Hospitalizations leave room for increased chances of negligence or adverse events from occurring. More research in this area must be done.
Acknowledgments
I thank Mentoring in Medicine Inc. for providing the resources and leadership necessary to collect sufficient data for analysis and to synthesize this data into a coherent paper. I also thank Mr. Andrew Morrison and the MIM Leadership Team for coordinating the internship under which the paper was written and providing a timeline for its publication.
References
- Goguen David, J.D. “Medical Negligence.” Www.alllaw.com, Nolo, 11 July 2019, alllaw.com/articles/nolo/medical-malpractice/negligence.html
- Figueroa, José F et al. “Across US Hospitals, Black Patients Report Comparable Or Better Experiences Than White Patients.” Health affairs (Project Hope) vol. 35,8 (2016): 1391-8. doi:10.1377/hlthaff.2015.1426 https://pubmed.ncbi.nlm.nih.gov/27503962/
- Goodheart, Eric S. “TWO TIERS OF PLAINTIFFS: HOW NORTH CAROLINA’S TORT REFORM EFFORTS DISCRIMINATE AGAINST LOW-INCOME PLAINTIFFS.” North Carolina Law Review, vol. 96, no. 2, Jan. 2018, p. 512+. Gale Academic OneFile. https://scholarship.law.unc.edu/nclr/vol96/iss2/5
- “U.S. Census Bureau QuickFacts: United States.” Census Bureau QuickFacts, U.S. Census Bureau, 2010, www.census.gov/quickfacts/fact/table/US/PST045219.
- LaVeist, T.A. Disentangling race and socioeconomic status: A key to understanding health inequalities. J Urban Health 82, iii26–iii34 (2005). https://doi.org/10.1093/jurban/jti061
- Iceland John, Wilkes Rima, Does Socioeconomic Status Matter? Race, Class, and Residential Segregation, Social Problems, Volume 53, Issue 2, 1 February 2006, Pages 248–273, https://doi.org/10.1525/sp.2006.53.2.248
- Wong LE, Hawkins JE, Langness S, Murrell KL, Iris P, Sammann A: Where are all the patients? Addressing Covid-19 fear to encourage sick patients to seek emergency care. NEJM Catalyst 2020; Online only: 1–12. https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0193
- Gold JAW, Wong KK, Szablewski CM, et al. Characteristics and clinical outcomes of adult patients hospitalized with COVID-19—Georgia, March 2020. MMWR Morb Mortal Wkly Rep 2020;69:545–50. https://www.cdc.gov/mmwr/volumes/69/wr/mm6918e1.htm
- Garg S, Kim L, Whitaker M, et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019—COVID-NET, 14 states, March 1–30, 2020. MMWR Morb Mortal Wkly Rep 2020;69:458–64. https://www.cdc.gov/mmwr/volumes/69/wr/mm6915e3.htm
- Ma QX, Shan H, Zhang HL, Li GM, Yang RM, Chen JM. Potential utilities of mask-wearing and instant hand hygiene for fighting SARS-CoV-2. J Med Virol. 2020;31:31. doi:10.1002/jmv.25805 https://pubmed.ncbi.nlm.nih.gov/32232986/
- Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ 2020;369. Epub May 22, 2020. 10.1136/bmj.m1966 https://pubmed.ncbi.nlm.nih.gov/32444366/
- Brennan TA, Hebert LE, Laird NM, et al. Hospital Characteristics Associated With Adverse Events and Substandard Care. JAMA. 1991;265(24):3265–3269. doi:10.1001/jama.1991.03460240061028 https://pubmed.ncbi.nlm.nih.gov/2046108/
